
As mentioned in our previous blog, Protection of the Eye in Patients With Facial Paralysis – Part 1, one of the most important priorities is to protect the cornea of the eye. In patients who present early in their paralysis (preferably within the first 6 to 12 months), reinnervation of the muscles of the face, particularly the orbicularis oculi muscle surrounding the eye, has been shown to provide superior protection to the cornea.
Nevertheless, because reinnervation takes time, most patients will still need “static” procedures, which further help in eye closure. These static procedures include both the upper and lower eyelids. Upper eyelid procedures mostly involve weighting of the upper eyelid, which is commonly performed with a gold or platinum weight or with fat grafting. Lower eyelid procedures may involve lifting the lower eyelid by either tightening, shortening, supporting with a small fascia graft, or a combination of the latter two. These procedures are also performed in patients who have long-standing facial paralysis of more than 18 months in which reinnervation of the facial muscles yields less optimal results. Below are some more details about these procedures.
Insertion of a Gold or Platinum Weight Into the Upper Eyelid
The principle of inserting a small weight in the upper eyelid has been utilized for many years. Many patients are concerned about this procedure since, traditionally, a bulge in the upper eyelid is seen as a result of the weight. In 2013, we published an article in the Journal of Plastic and Reconstructive Surgery on how to place the weight in a more hidden and discrete position in the eyelid. This newly described procedure, which was adopted by many centers in the world, has several advantages:
- The weight is significantly less visible than in the traditional technique. It does not distort the eyelid aesthetic landmarks, and in most patients, it’s difficult to identify at talking distance.
- The chances of extruding through the skin are minimized since it is covered not only by the skin but also by muscle, septum (hence the term post-septal technique), and fat.
- The chances of abnormal ptosis (having the upper eyelid too low in the resting position) are significantly reduced.
By using this technique of weight placement, patients benefit from improved function and aesthetics. For further details, Figures 1 to 2 provide some information on the technical aspects of the procedure.
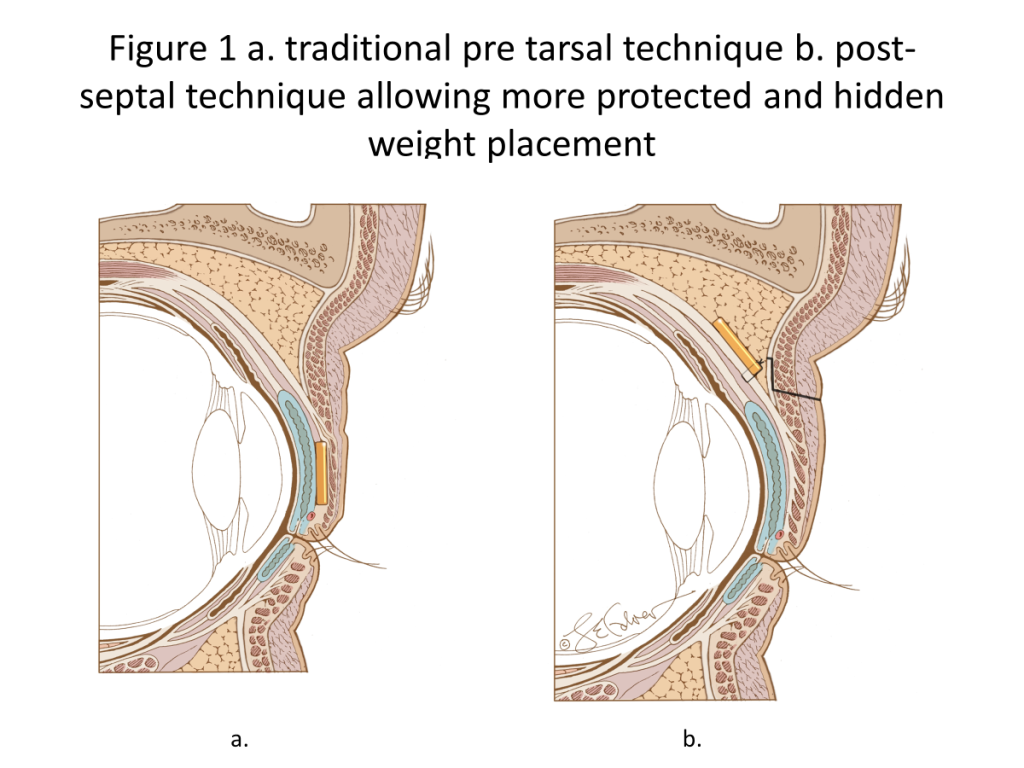
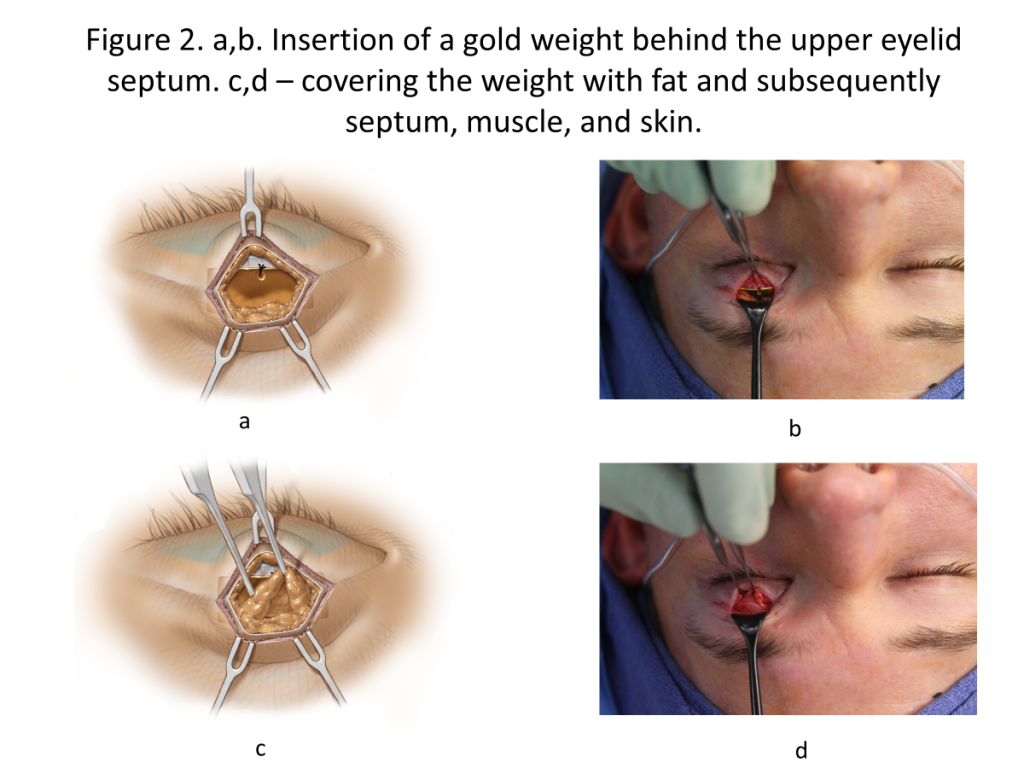
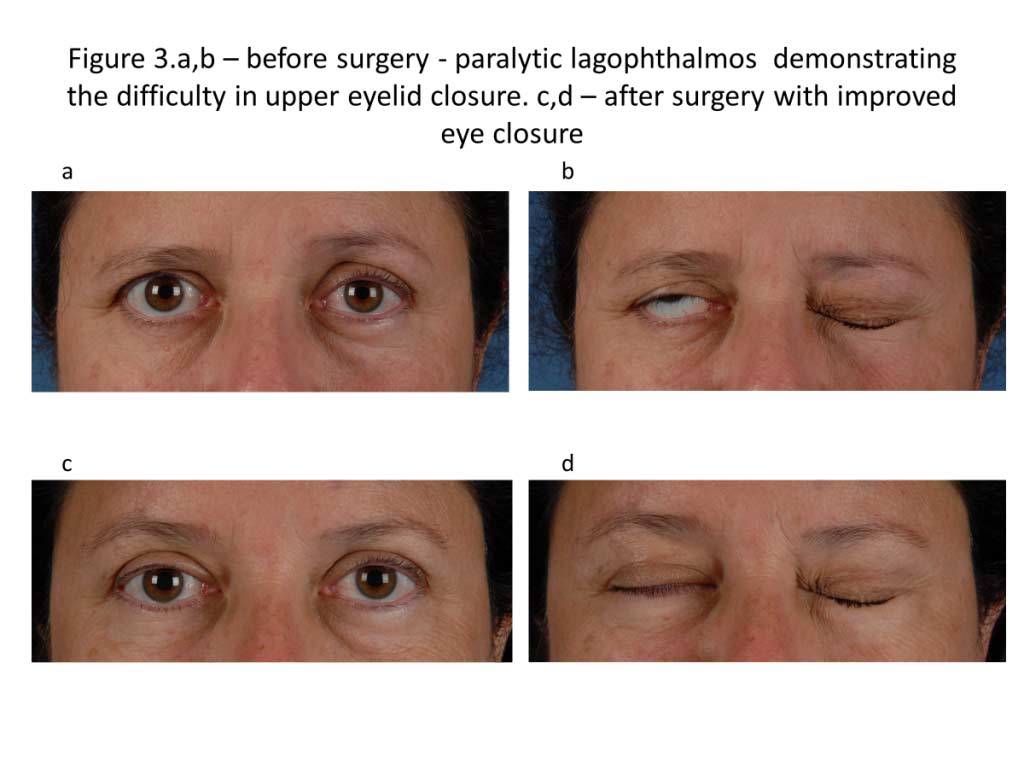
Figure 3 provides before and after images of a patient with better eye closure after post-septal upper eyelid gold weight placement.
For more in-depth reading about the insertion of a weight in the upper eyelid, we provided you with a link to the abstract (Rozen S*, Lehrman C. Upper eyelid post-septal weight placement for treatment of paralytic lagophthalmos. Plast Reconstr Surg. 2013 Jun; 131(6):1253-65. PMID: 23714789. DOI: 10.1097/PRS.0b013e31828be961).
Lower Eyelid Support Procedures
The lower eyelid is often affected in facial paralysis and is lower than it should be—a condition called paralytic ectropion. Although most of the motion of the eyelids is in the upper eyelid, the position of the lower eyelid is very important for both corneal coverage and proper tear drainage.
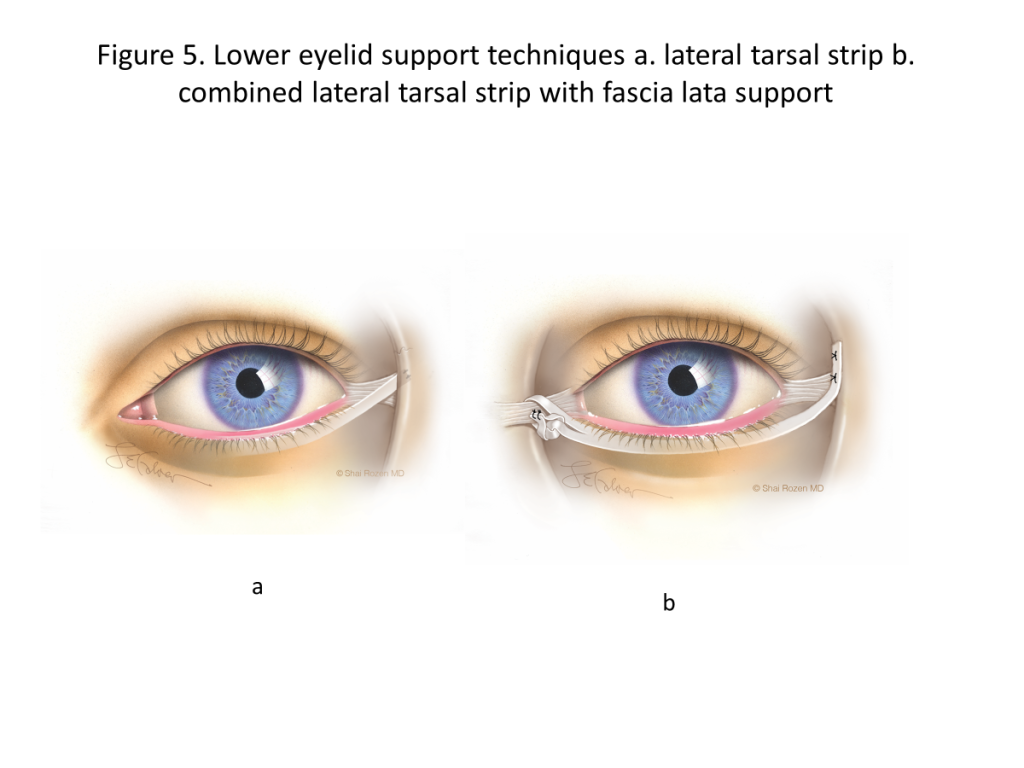
Traditionally, the lower eyelid is repositioned to the side and upward, a procedure termed canthoplasty. If the eyelid needs to be slightly shortened at the same time because of laxity, the procedure is called a lateral tarsal strip. Both of these procedures are good when used in the correct patients, but the main problem frequently encountered with them is that they pull the eyelid too far to the side, distort the appearance, and cause the medial punctum (a small hole in the inner part of the eyelid which drains the tears), to be pulled sideways.
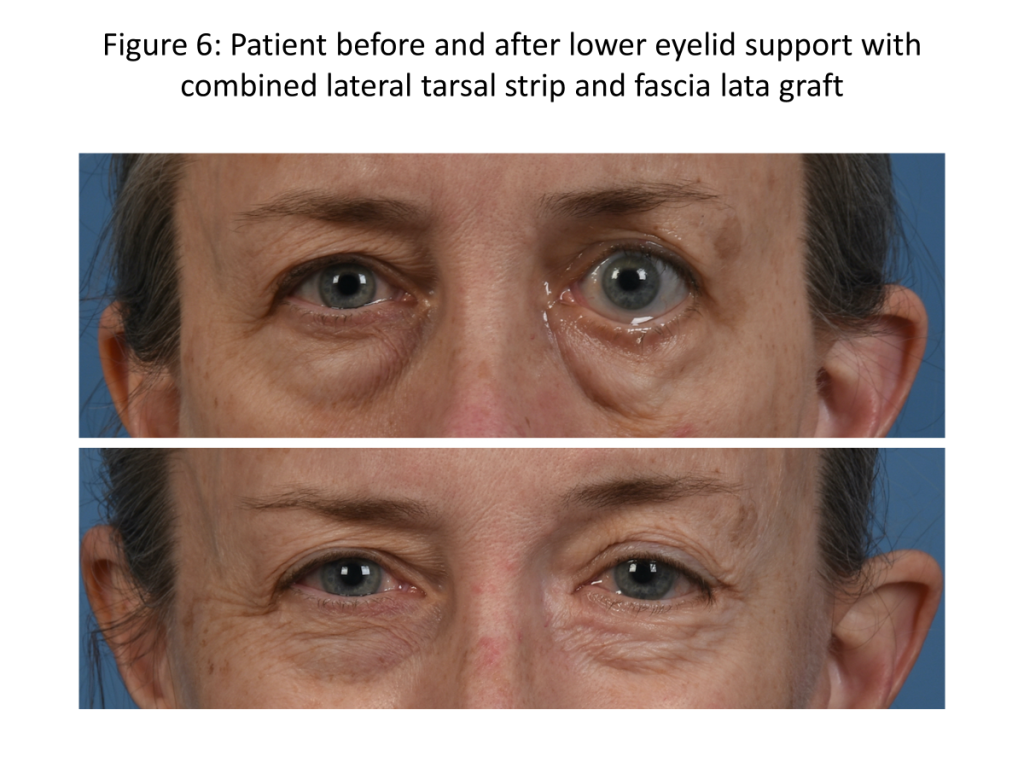
In 2022, we modified a technique in which a small piece of fascia from the thigh was used to support the lower eyelid in addition to the procedure noted above. This allowed a more evenly distributed lift of the lower eyelid, providing a more symmetric lift to both the medial and lateral portions of the lower eyelid without pulling the medial punctum to the side. Below are some figures describing the technique, followed by a link to the article.
For more in-depth reading about lower eyelid support techniques, we provided you with a link to the abstract (Sanchez CV, Thachil R, Mitchell DN, Reisch JS, Rozen SM*. Lateral Tarsal Strip versus Tensor Fascia Lata Sling for Paralytic Ectropion – Comparison and Long-Term Outcomes. Plast Reconstr Surg. 2023 Apr 13. PMID: 37053441. DOI: 10.1097/PRS.0000000000010533).
In summary, weighting of the upper eyelid and supporting of the lower eyelid are critical treatment strategies for the paralyzed eyelids and are essential to protect the cornea and prevent blindness. At the same time, it is critical and as important to obtain an aesthetic result that restores and provides facial symmetry and harmony.
Read Part 1 of this blog post to learn more about nonsurgical eye protection treatments and why protecting the cornea is important. For more information about eye closure and protection related to facial paralysis, request a consultation to meet with Dr. Rozen at UT Southwestern.
Leave a Reply